
Gestational diabetes (GDM) is a common diagnosis received during pregnancy. It affects between 3-20% of pregnancies, causing higher blood sugars than normal during the pregnancy period.
The good news is that blood sugars will return back to normal within a few hours after delivery for most women!
The temporary nature of gestational diabetes makes it a little different than other forms of diabetes, such as Type 1 or Type 2 diabetes which can be more chronic and/or lifelong.
Read on to find out what causes these high blood sugars and what can you do to effectively manage your blood sugars with gestational diabetes.

Adalia Yang
What Causes Gestational Diabetes?
First and foremost, gestational diabetes is not your fault.
It is a common misconception that diabetes, including gestational diabetes, are caused by eating too much sugary foods and/or too much carbs. Gestational diabetes are mainly caused by hormonal changes that happen during pregnancy.
During pregnancy, the placenta produces certain hormones (estrogen, cortisol, and human placental lactogen) that helps the baby grow and develop.
These hormones interfere with how the body from effectively using insulin, leading to insulin resistance.
Insulin is the hormone that helps our body use the sugar (glucose) from our blood. Glucose is an essential source of energy for our brain, muscles, and organs.
Placental hormones start to rise week after week until about 36 weeks and as a result of these rising hormones, blood sugar level increases.
To compensate, the body will try to produce more insulin. But in some cases, especially if the body can’t keep up with this increased demand, this can lead to gestational diabetes.
You are more at risk for developing gestational diabetes if you are :
- age of 35 or older,
- ethnicity (African, Arab, Asian, Hispanic, Indigenous or South Asian),
- obesity,
- previous diagnosis of GDM,
- history of prediabetes,
- had a large baby (> 4kg) in a previous pregnancy,
- family history of type 2 diabetes,
- use of corticosteroids,
- polycystic ovarian syndrome
Gestational Diabetes Symptoms
There are usually no symptoms which makes screening especially important but some women may experience increased thirst, increased hunger, and blurred vision.
When to Test for Gestational Diabetes?
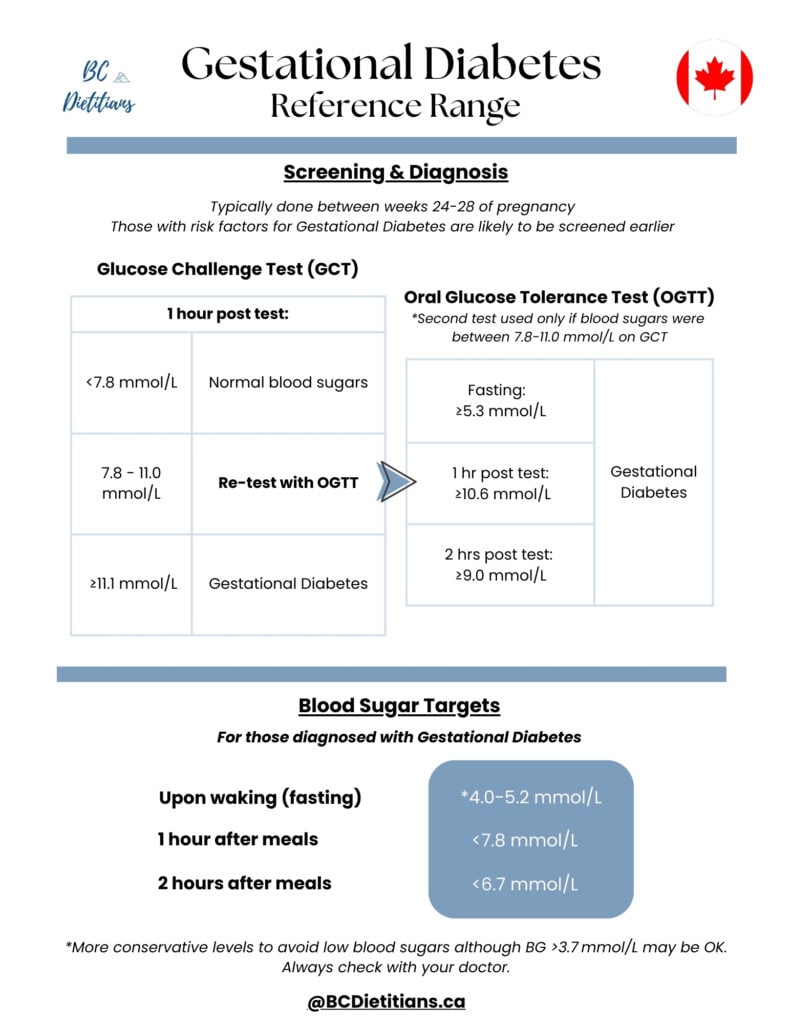
Screening for gestational diabetes happens around ~24-28 weeks of pregnancy.
You may be screened earlier if you have had GDM in a previous pregnancy or have some of the above risk factors. The screening process involves check your blood sugars and monitoring your body’s response to sugar after 1 and/or 2 hours in an oral glucose tolerance test (OGTT).
- You will complete a blood before and 1 hour after taking an orange sugary drink. This measure shows how your body responds to sugar.
- If the results show high blood sugar levels, you will complete a second test with a drink that contains more sugar and your blood sugar will be checked three times:
(1) before drinking the beverage, (2) at the 1 hour mark, and (3) at the 2 hour mark.
- GDM is diagnosed if one of these values is abnormal at the second test:
fasting blood sugar ≥5.3 mmol/L,
1 hour blood sugar ≥10.6 mmol/L,
2 hours blood sugar ≥9.0 mmol/L - Some women may only complete the 75 g oral glucose tolerance test (to avoid the extra testing).
- GDM is then diagnosed if one of these value is abnormal :
fasting blood sugar ≥5.1 mmol/L,
1 hour blood sugar ≥10.0 mmol/L,
2 hours blood sugar ≥8.5 mmol/L - Women who are diagnosed with gestational diabetes will be referred to a diabetes clinic with doctors or endocrinologists, nurses, dietitians, and diabetes educator to provide comprehensive care. This referral process can take several weeks.
Book an appointment with a diabetes dietitian if you’d like to get started right away in a personalized nutrition plan to manage your gestational diabetes.
How does Gestational Diabetes affect the mother and baby?
Gestational diabetes can affect both the mother and baby, particularly when the high blood sugars are not well managed:
- Impact on Mother:
- Increased risk for preeclampsia
- Increased risk for C-section
- Increased risk for preeclampsia
- Impact on Baby:
- Baby may grow to be larger than normal. This can cause injury during birth and a c-section may be required to safely deliver the baby
- Baby may develop low blood sugar shortly after being born. If the mother’s blood sugars were high in pregnancy, the baby will continue to produce extra insulin for several hours after birth, causing blood sugars to become low. They may be given extra sugar to bring blood sugar levels back to normal
- Respiratory issues
- Jaundice
- Increased risk for developing type 2 diabetes and obesity in adulthood
- Baby may grow to be larger than normal. This can cause injury during birth and a c-section may be required to safely deliver the baby
How is Gestational Diabetes Treated?
Gestational diabetes is managed through a combination of nutrition, exercise, monitoring your blood sugars and sometimes medication(s):
- Checking blood sugars – you will need to check and monitor your blood sugars frequently throughout the day, either through finger pricking and/or continuous glucose monitoring (CGM).
- Once you start to understand your individual pattern and how your body respond to carbs and sugars. You can then work with a registered dietitian on a personalized gestational diabetes diet (ie. step #1)
- Exercise can be an effective way to use up some of the carbs for energy and help lower blood sugars, especially after a meal
- Medications such as insulin, may be needed and prescribed by your doctor, OBGYN and/or endocrinologist
What is the Diet for Gestational Diabetes?

Nutrition is one of main strategies to manage gestational diabetes.
Your first response to a GDM diagnosis may be to limit intake of carbohydrates and sugar with the goal of reducing blood sugar. However, this is not recommended in pregnancy as carbohydrates provide necessary energy to the mother and baby.
The key is to manage the portion size and timing of carbohydrate intake to prevent high blood sugars.
For example, eating a large portion of carbohydrates in one sitting will cause blood sugar levels to rise quickly and become very high. It will take a substantial amount of time for the blood sugar to come back down to normal levels as your body tries to produce enough insulin to use the sugar.
In contrast, if the carbohydrate intake is spread out throughout the day and the portion is smaller, your blood sugar levels will stay within the normal range and both the mother’s and baby’s nutrient needs can be met.
A dietitian will work with you to create a balanced meal plan that meets your daily carbohydrate and nutrition needs while keeping your blood sugars in range.
We typically work through these nutrition strategies with our clients :
- Aim for 3 meals and 1-3 snacks per day
Meals: follow the plate model as a guide for breakfast, lunch, and dinner –
- ¼ plate of carbohydrate foods : starchy vegetables (potatoes, plantains, yams, carrots, corns, green peas, pumpkin, beets, taro), grains, fruit, milk, yogurt, and legumes
- ¼ plate of protein foods : animal meat, fish, seafood, tofu, nuts/nut butters, seeds, eggs, cheese, milk*, yogurt*, and legumes*
- ½ plate of non-starchy vegetables : lettuce, broccoli, cauliflower, celery, tomatoes, mushrooms, zucchini, leafy greens, cabbage, peppers, eggplant, asparagus, etc.
Snacks: Pair carbohydrates with protein. Protein slows down our digestion and absorption of sugar from food.
Some examples of the pairings include –
- 1 apple + 1 egg
- ½ banana + 1 tbsp peanut butter
- 100g yogurt*
- ~4 crackers + 1 slice cheese
- 1 slice toast + 1 slice cheese
*These foods are both a carbohydrate and protein source.
2. Choose whole grain options over the refined alternative at least 50% of the time.
Whole grains contain fiber which slows down digestion and our body’s absorption of sugar from food. Whole grains include: brown rice, whole grain bread, quinoa, whole grain pasta, oats.
3. Space meals 4-6 hours apart and snacks at least 2 hours apart from meals.
This timing will allow blood sugars to come down before the next meal or snack. For example, a sample eating schedule may have breakfast at 8am, lunch at 12pm, snack at 3pm, dinner at 6pm, snack at 10pm.
Here are some additional resources on nutritional strategies to manage blood sugar:
- Carb counting – In pregnancy, the goal is to eat a minimum of 175g or 12 carbohydrate servings per day. This is typically spread out over 3 meals and 1-3 snacks.
- Sample meal plan for gestational diabetes from Diabetes of Canada
- Glycemic Index– Choose foods with low glycemic index more often as they result in a lower blood sugars compared to high glycemic index foods.
4. Increase exercise : muscles use sugar in the blood as fuel when you’re exercising.
Incorporating exercise, especially immediately after a meal, can help you lower your blood sugar at the 1 hour mark. Even low-impact exercises such as walking for 10-15 minutes after a meal can be very effective (lowered by 1mmol/L)!
*Note: exercise may not safe for all pregnancies, please speak to your doctor before making drastic changes to your exercise routine.
5. Medication : If blood sugar levels stay above safe levels with nutrition and lifestyle changes, your healthcare team may recommend insulin and/or another type of medication to help lower your blood sugar.
Insulin is safe in pregnancy and is delivered through a small injection, usually to the side of the stomach. As the pregnancy progresses, more insulin may be required as the placenta continues to produce more hormones.
Will Gestational Diabetes Go Away?
The mother’s blood sugar should return to normal shortly after birth.
If the mother is taking insulin, insulin will either no longer be required or the dose significantly reduced until blood sugars return to normal.
Baby’s blood sugar may become lower than normal after delivery (see above section on What Are the Risks of Gestational Diabetes?). They may require additional sugar, typically delivered orally or through a needle.
Gestational Diabetes to Diabetes
With a gestational diabetes diagnosis, you do have a higher risk of developing type 2 diabetes in the future. To decrease risk of developing type 2 diabetes, mothers can:
- Breastfeed for a minimum of 4 months whenever possible. This reduces both the mother’s and baby’s risk of developing type 2 diabetes in the future.
- Monitor blood sugar levels to rule out type 2 diabetes:
- Take another oral glucose tolerance test within 6 weeks to 6 months after delivery
- Screen for diabetes every 3 years or more often if recommended by doctor
- Take another oral glucose tolerance test within 6 weeks to 6 months after delivery
- Continue eating balanced meals and snacks (e.g. plate model or Canada’s Food Guide)
- Gradually start regular exercise again (wait at least 6 weeks after delivery and clearance from your doctor), eventually work up to ~150 minutes of moderate-vigorous physical activity per week plus resistance training twice a week.
- Achieving and maintaining a healthy weight after you have recovered from delivery
The recommendations provided in this blog post are meant to provide you with general information and suggestions. Please follow your care provider’s recommendations as they know your specific situation best and consult your care provider before making any significant dietary and lifestyle changes.
References
- Diabetes Canada Clinical Practice Guidelines Expert Committee. Diabetes Canada 2018 Clinical Practice Guidelines for the Prevention and Management of Diabetes in Canada: Diabetes and Pregnancy. Can J Diabetes. 2018;42(Suppl 1):S1-S325
- Lipsombe L, Booth G, Butalia S, Dasgupta K, et al. Diabetes Canada 2018 Clinical Practice Guidelines for the Prevention and Management of Diabetes in Canada: Pharmacologic Glycemic Management of Type 2 Diabetes in Adults. Can J Diabetes 2018;42(Suppl 1):S88-S103
- Health Link BC. (Updated 2023). Gestational Diabetes. Accessed from: (https://www.healthlinkbc.ca/pregnancy-parenting/pregnancy/your-health-during-pregnancy/gestational-diabetes
- Health Canada. (2018). Physical Activity Tips for Adults (18-64 years). Accessed from: https://www.canada.ca/en/public-health/services/publications/healthy-living/physical-activity-tips-adults-18-64-years.html






Add a comment