
Kidney disease impacts 1 in 10 Canadians, with more than 53,000 Canadians currently being treated for kidney failure.
The North Western Renal Dietitians Conference 2026 took place on March 5 – 6, 2026 with the theme “Flavourful Paths to Kidney Health: Celebrating Chinese Cuisine & Cultures.” Dietitians and healthcare professionals gathered to discuss nutrition care through a cultural lens of traditional Chinese cuisine for chronic kidney disease (CKD).
Over the two-day event, attendees heard from several experts in renal health. BC Dietitians were also invited to present a research poster.
Private Practice Dietitians can Bridge the Gap
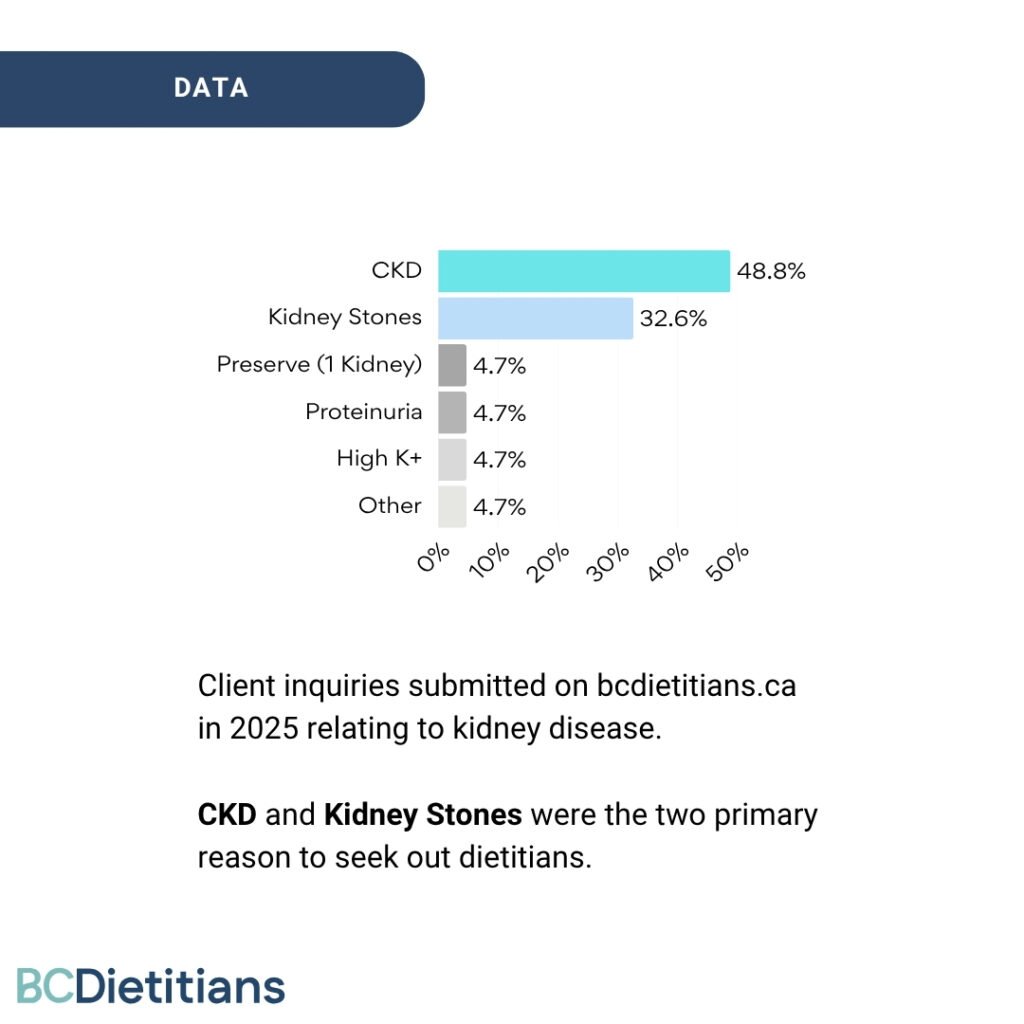
BC Dietitians analyzed kidney-related inquiries submitted on our website in 2025.
Nearly 48.8% of the inquiries were related to CKD, followed by 32.6% for kidney stones.
We found that private practice dietitians can help bridge this gap by providing early nutrition support for patients in CKD stages 1–3a, as well as care for related conditions that may not be referred to Kidney Care Centers (KCC), such as kidney stones or patients with higher eGFR and other health conditions like diabetes or heart disease.
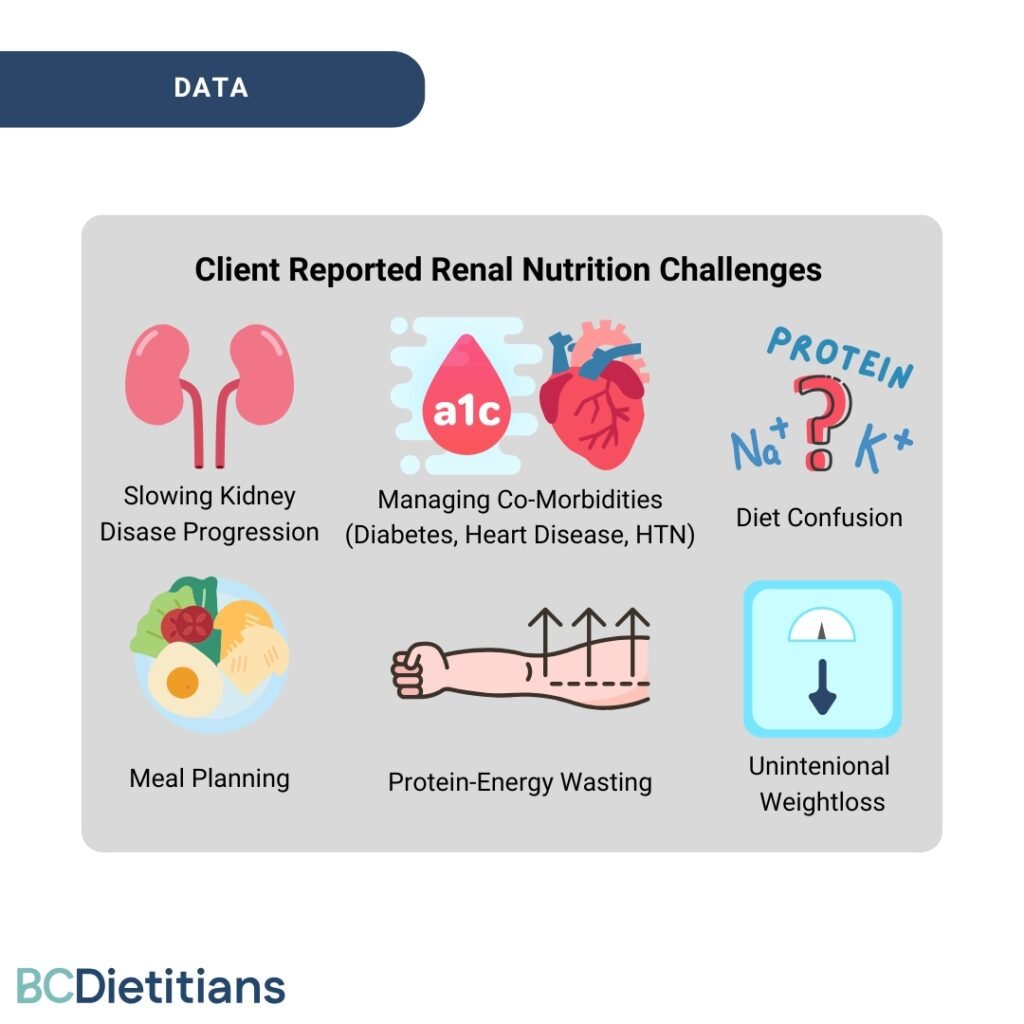
Key Nutrition Challenges Identified from the Renal-Related Client Inquiries:
- Proactively slowing progression of kidney disease
- Managing co-morbidities (diabetes, heart disease, HTN)
- Diet confusion (K+/PO4/Protein)
- Meal planning
- Protein energy malnutrition
- Unintentional weight loss
Many patients reported confusion about kidney diets and relied on outdated food lists found online. This often led to unnecessary over-restriction (especially protein, potassium and phosphorus), malnutrition and significant unintentional weight loss.
Patients with early CKD stages 1-3a are managed by their primary provider and can access general nutrition support through outpatient services like HealthLink BC.
Once a patient’s disease progresses to stage 3b+, they are referred to a nephrologist who can then refer the patient to a Kidney Care Clinic (KCC) to access a renal dietitian.
However, the wait time from diagnosis to seeing a nephrologist and/or renal dietitian is at least 18 months.
Early nutrition intervention with a private practice dietitian can help:
- Slow CKD progression
- Prevent unnecessary dietary restrictions
- Reduce the risk of malnutrition
- Support management of complex comorbidities (diabetes, hypertension, heart disease)
Healthcare providers can help close the gaps in early CKD nutrition care by referring patients to a private practice dietitian in early stages and while they wait for specialized care.
Many people in British Columbia have extended health insurance coverage that includes dietitian services.
Updates on Kidney Nutrition
We also had the honor of learning from the experts in the field on CKD and the Chinese Cuisine and Culture. The annual NWRD conference brings together registered dietitians to inspire, support and educate on improving the lives of those living with CKD.
“The Chinese Soup Tradition: Cultural Significance and Renal Nutrition Implications” by Beverley Lau, RD and Vicky Ngo, RD.
Food carries deep cultural meaning and an example is Traditional Chinese Soup which is used as preventative medicine, rooted in the principle of maintaining balance between yin and yang. Additionally, food brings families and communities together, offering comfort, connection and a sense of tradition.
Traditional Chinese soup typically includes three components: an animal protein, dried herbal ingredients, and leafy or root vegetables, and is served as part of a regular meal.
The speakers highlighted the importance of respecting traditional cuisines while making thoughtful adaptations to align with renal nutrition guidelines. Such as reducing the amount of high potassium/phosphourous dried ingredients such as lotus seeds, white fungus, and dried scallops. As well as limiting soup intake to 250mL/day.
“Balancing Blood Sugar and Kidney Function with a Chinese Cultural Lens” by Daisy Lin, RD
Diabetes is the leading risk factor for chronic kidney disease (CKD), followed closely by hypertension, highlighting the strong link between CKD, diabetes, and heart disease.
Managing blood glucose (target A1C <7.0%) can help reduce the risk and slow the progression of CKD. High blood glucose may also raise serum potassium levels, which can be dangerous for patients whose kidneys cannot effectively remove potassium.
The presentation emphasized the importance of culturally appropriate nutrition education, as it can improve patient knowledge, self-management, behavior change, and clinical outcomes.
Daisy also covered how a Continuous Glucose Monitor (CGM) can be used to support diabetes management by providing real-time data that helps patients understand how food choices and habits —such as adding protein or fiber to carbohydrates or taking a walk after meals—affect their blood sugar.
“Ethical Considerations in End-of-Life Care” by Jennifer A. Gibson, RN, MSN, PhD
Jennifer explored the Ethical Considerations in End-Of-Life Care and how dietitians can apply the four principles of ethics in healthcare–autonomy, beneficence, non-maleficence, and justice—to guide nutrition decisions. For dietitians, this typically entails supporting individuals who choose to “eat at risk” and meeting the patient where they are in their care goals. This involves clear communication of identified risks and mitigation strategies to support informed patient choice. Nutrition interventions should be effective while remaining the least restrictive and least intrusive to the patient’s quality of life.
“The Interface between Chinese Culture and Western Medicine and Medication Management in CKD” by Dr. Claudia Ho, Clinical Pharmacy Specialist at Fraser Health
Traditional Chinese medicine (TCM) emphasizes prevention, wellness, and restoring balance in the body. It may include natural remedies such as herbal medicines or practices like acupuncture. However, some TCM therapies may pose safety risks for renal patients, particularly due to potential interactions with the organ graft or kidney medications. Dr. Claudia Ho echoed the previous presentation on ethics presented by Jennifer A. Gibson, on the importance of respecting patient autonomy and working collaboratively to safely integrate TCM into a renal care plan when appropriate.
“Considerations GLP-1 Receptor Agonists in CKD” by Joseph Fonseca, RPh
Clinical pharmacist Joseph Fonseca highlighted that GLP-1 receptor agonists (GLP-1RA) may be added when SGLT2 inhibitors are insufficient for glycemic management. In addition to lowering blood glucose, GLP-1RA reduces weight, blood pressure, and serum lipids, which can indirectly benefit kidney health and highlights the interconnection between CKD, diabetes and heart disease. When initiating or increasing the dose, patients commonly experience gastrointestinal side effects such as nausea, vomiting, diarrhea, or constipation. Patients are encouraged to continue the medication for 2–4 weeks, as symptoms often improve. Dietary recommendations for managing the strong GI side effects are similar for gastric reflux and include eating slowly, small frequent meals that are nutrient dense and avoiding food triggers.
Chinese Food Cooking Demo by Renee Chan, MS, RD, MBA, RYT & Chef of The Skript Kitchen
The cooking demonstration from Skript Kitchen Founder Renee Chan, RD, also discussed the use of TCM ingredients as part of Chinese cuisine. We got to sample a sweet soup made with astralagus radix, goji berries, cordyceps flower and chinese red dates. As well as a stirfry of rhizoma dioscoreae (chinese yam) and lotus bulbs. The ingredients provide not only nutritional benefits, but can also have protective health effects.
Final Thoughts
During the NWRD 2026, we heard from experts in renal health and the pivotal role dietitians have in providing culturally safe care. It deepened our understanding on creating nutrition interventions that honour Chinese culture and cuisine for people living with kidney diseaess.
There is a missed opportunity in early nutrition intervention and private practice dietitians are well-positioned to support early stage CKD patients and patients with other kidney related conditions that would typically not be referred to a KCC.







Add a comment